In some cases, tension can also be generated in muscle without muscle stretching. Hence, the process of generation of tension within muscle fibers in order to generate force to do any physical activity can be defined as muscle contraction.
Muscle contraction occurs when there is movement in any part of our body; like when we perform any physical activities or when any internal organ of our body is physically functioning. Muscle contraction of skeletal muscles can be controlled according to our will; whereas, contraction of smooth and cardiac muscles are involuntary. Contractions of skeletal muscles are neurogenic i.e. they are initiated by nerve impulses. On the other hand, cardiac muscle contraction and smooth muscle contraction are myogenic in nature i.e. their contractions are initiated within the muscle cells.
Table of Contents
Interesting Science Videos
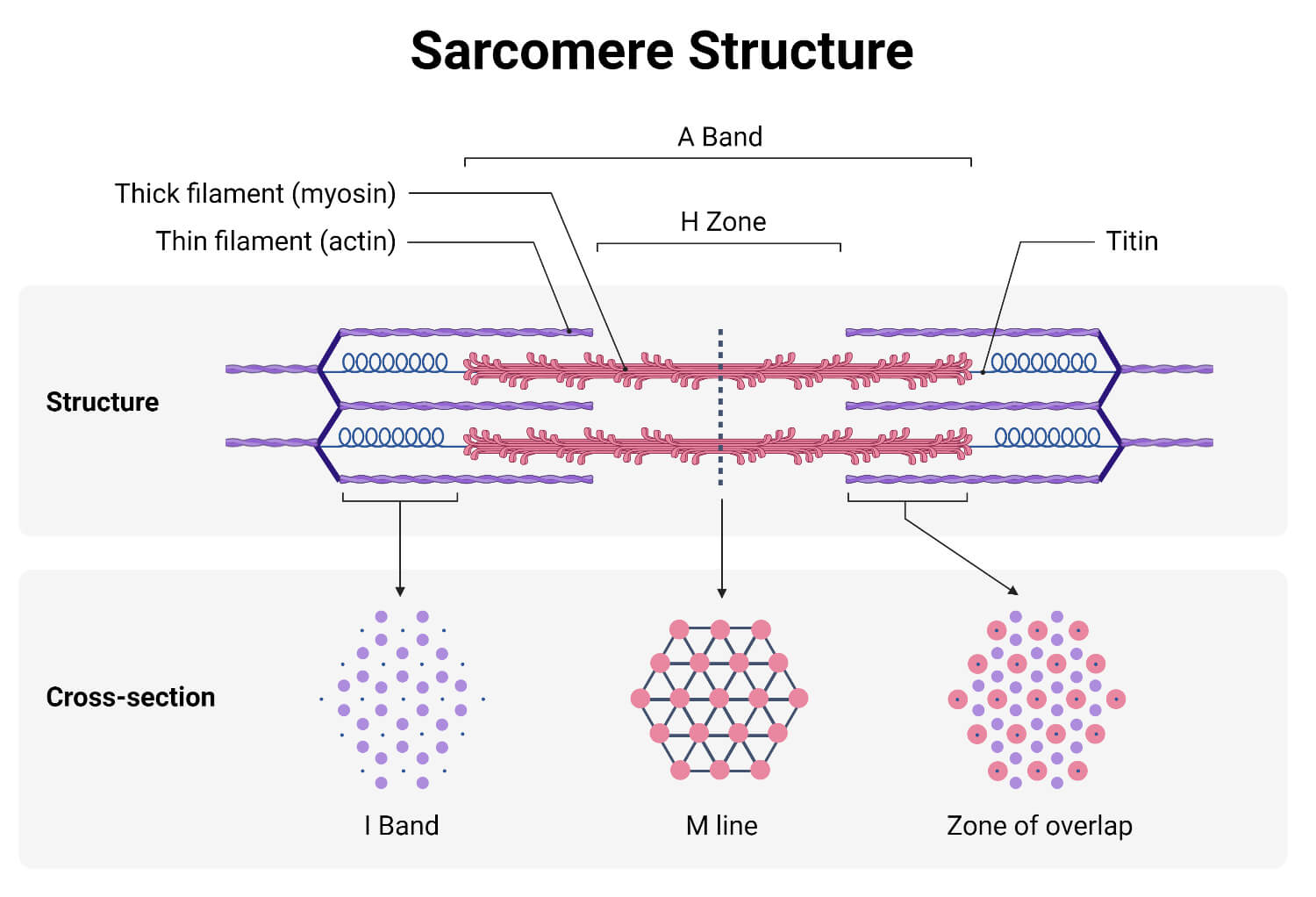
Two proteins, namely actin and myosin are responsible for muscle contraction. These proteins form a thick and thin band of myofilaments, which together forms a sarcomere.
Actin is a family of globular proteins forming thin filaments, one of the important structures in muscle fibers. They are present as either free monomeric protein or may be combined in form of thin micro-filament. In both form they are very important in muscle contraction. Actin molecules together with tropomyosin and troponin proteins form an actin myofilament. Two actin filaments cover a myosin filament. During muscle contraction, the myosin fiber moves along the actin filaments, reducing the length of the muscle fiber.
Myosin is a family of motor proteins responsible for actin-based motility of muscle fibers. A myosin molecule is composed of three domains; head, neck, and tail. The head binds to actin and using ATP hydrolysis, contract the muscle fiber.
Based on the change in muscle tension and muscle length, muscle contraction can be differentiated into following four types;
In this type of contraction, there is change in muscle tension without change in muscle length. For instance, during grabbing something, muscles in forearm experience increase in tension, but there is no change in length of muscle of the forearm.
In this type of contraction, there is change in muscle length without change in muscle tension. For instance, when carrying load equal to muscle tension generated in forearm muscle, there is isotonic contraction in forearm muscle.
In this type of contraction, there is shortening of muscle length while generating muscle tension. For instance, while carrying heavy load, the muscle in biceps shorten but tension is generated in the biceps muscles.
In this type of contraction, there is increase in the length of the muscle along with generation of muscle tension. For instance, while lowering the arm while carrying a heavy load, eccentric contraction occurs in the biceps muscles.
There are four main mechanisms proposed, explaining how the muscle contraction is initiated and caused. These mechanisms are described below in brief:
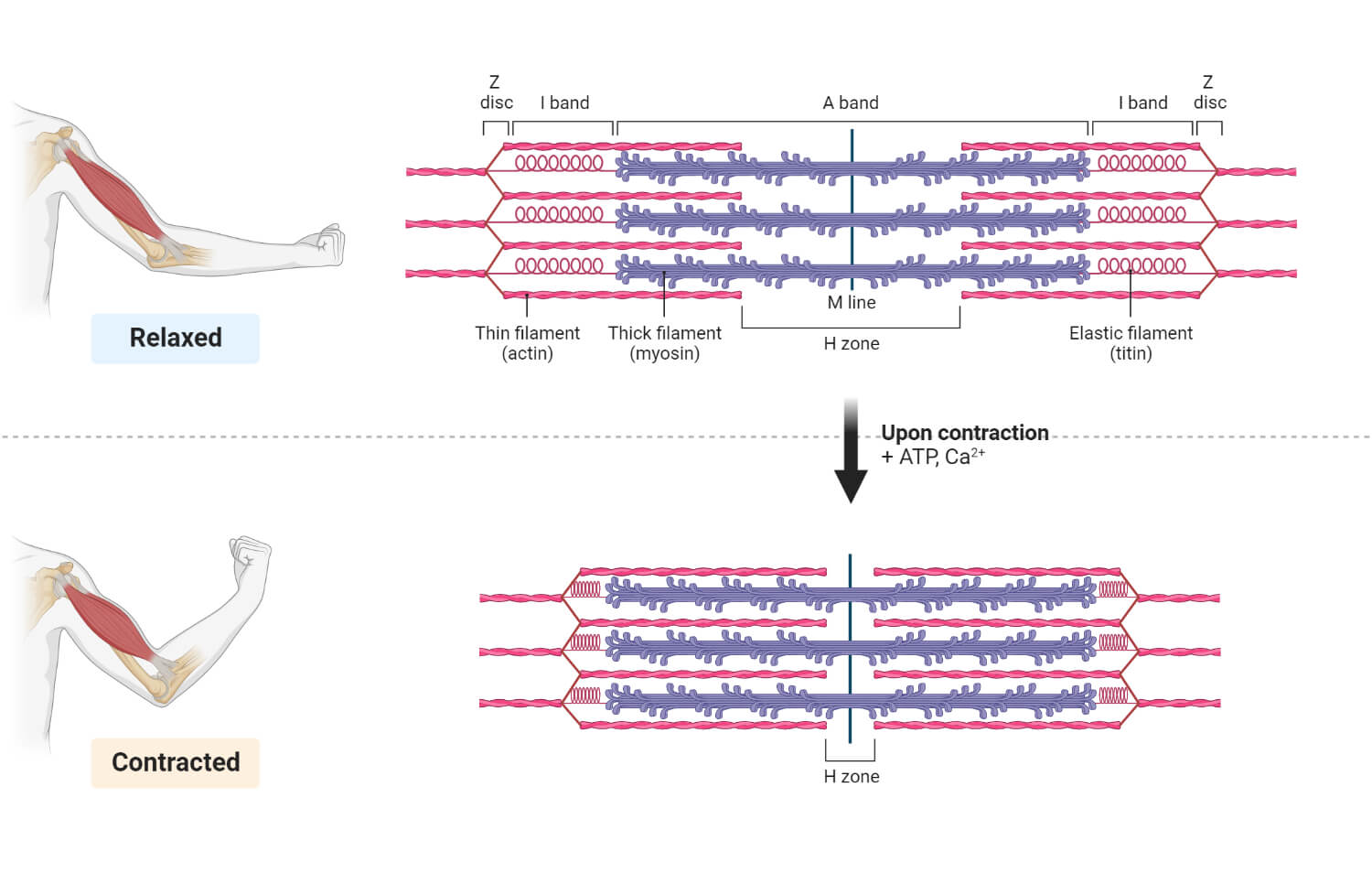
This is a widely accepted theory explaining mechanism of muscle contraction which has been regarded as the most accurate theory with support from results of numerous experiments. This mechanism was first proposed by Huxley and Hanson in 1954.
This mechanism claims that muscle fibers contract by sliding of the actin filaments over the myosin filaments within a myocyte. (The above mentioned general steps of muscle contraction are based on this theory.) During muscle contraction, the myosin heads attach to the actin filaments and form a cross-bridge. The myosin head then pulls the actin filaments towards the center of sarcomere using energy generated from hydrolysis of ATP molecule. This results in the shortening of the sarcomere and contraction of muscle fiber generating muscle tension. After muscle contraction, the myosin head detaches from the actin filament and the sarcomere returns to its original resting length.
This theory states that action potential in a myocyte triggers the release of Ca ++ ions from the sarcoplasmic reticulum, leading to the muscle contraction. This theory was first proposed by Ringer in 1882.
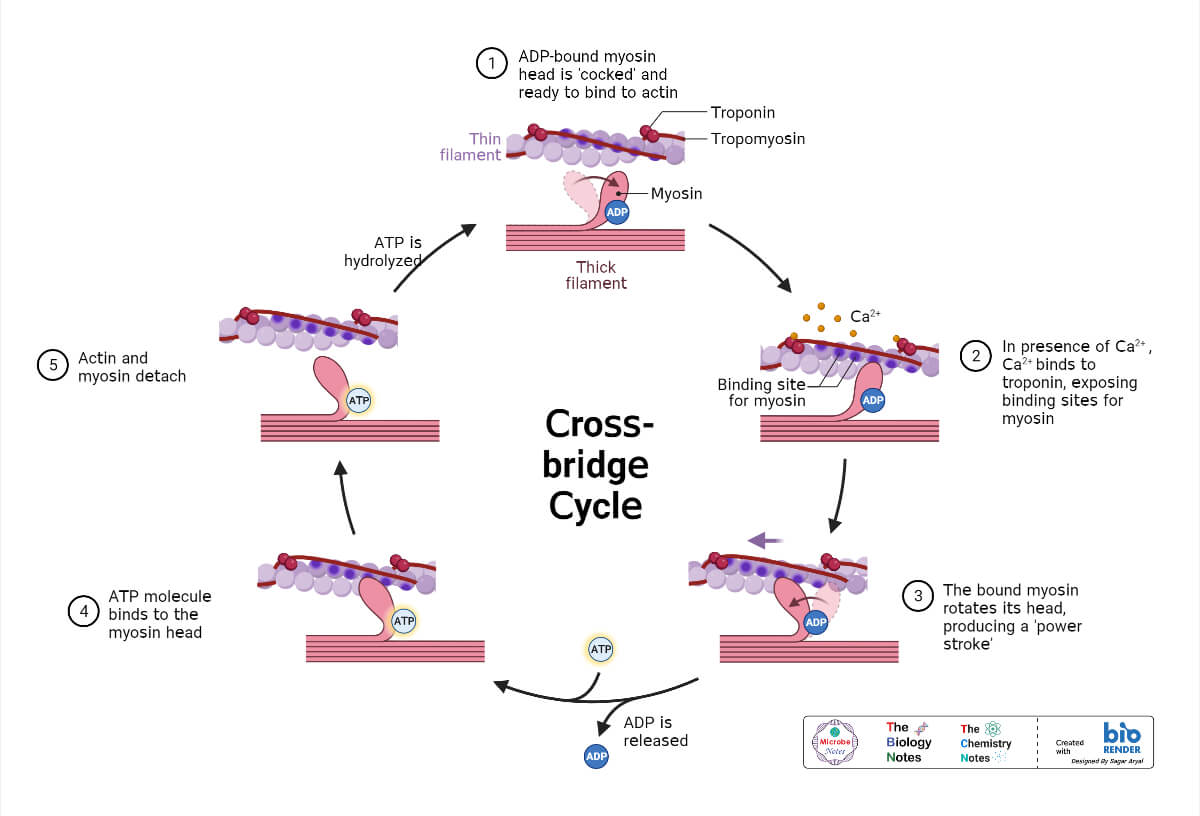
The action potential reaches the muscle cell and into the T-tubules. This triggers the release of Ca ++ ions from the sarcoplasmic reticulum into the cytoplasm of the myocyte. The released Ca ++ ions bind to the ‘troponin’ protein complex causing removal of ‘tropomyosin’ releasing the binding sites of myosin on actin filaments. The myosin head will then binds to the actin filaments, forms cross-bridge and initiate sliding mechanism.
This theory explains how a muscle fiber contracts by the recruitment of the additional motor units as the force required for the contraction of muscle is increased. This theory was first proposed by Granit in 1939.
Additional motor unit contains a motor neuron and the muscle fiber it innervates. When a muscle contraction is required, the nervous system sends impulses through motor neuron to stimulate their associated muscle fiber to contract. Initially, small motor units are activated and as more muscle contraction is needed (more muscular force is needed), larger motor units are activated until all available motor units are activated generating maximum needed muscle contraction. This process of gradually activating motor units is called “motor unit recruitment”.
This theory states that muscle contraction involves the activation of muscle fibers in response to a sudden stretch. This theory was first described by Sherrington in 1906.
When a muscle is stretched, sensory receptors in the muscle are sensitized, which send the signal of muscle stretch to the spinal cord. The spinal cord then sends back command to contract the muscle in order to resist the stretch. This type of muscle contraction is generally seen during reflex action and involuntary muscle movement.
About Author
Prashant Dahal completed his bachelor’s degree (B.Sc.) Microbiology from Sunsari Technical College, affiliated with Tribhuvan University. He is interested in topics related to Antimicrobial resistance, the mechanism of resistance development, Infectious diseases (Pneumonia, tuberculosis, HIV, malaria, dengue), Host-pathogen interaction, Actinomycetes, fungal metabolites, and phytochemicals as novel sources of antimicrobials and Vaccines.